Physical restraint has rightly been getting a lot of attention in recent years. Since the BBC Panorama programme on Winterbourne View in 2011 there has been an increased attention towards abusive practices. There are risks that physical interventions can be misapplied and used abusively. There are also significant risks of harm to people who experience physical restraint, such as death from positional asphyxiation, physical injuries and trauma.
This has led to a welcomed increased level of recording of physical interventions, which in turn is giving greater insight into how much physical interventions are being used in health and social care. The increased recording may potentially be giving a false impression that the use of restraint is increasing. However, the data continues to highlight this is an important area of health and social care that demands further attention.
Physical interventions and restraint is a highly emotive topic. It is easy to form very polarised views on the topic. This can lead to views such as “all physical interventions are bad” or “people who use physical interventions are abusive”. This polarisation can make it difficult to have sensible conversations on this hugely important issue.
Largely in response to the increased negative attention and the public disapproval of physical restraint the terms “restraint reduction”, “restraint elimination”, and “least restrictive” have gained support and increased usage. These are premise setting statements that no one would disagree with. However, as their usage has increased, I feel some of the practicalities of their application requires thought.
This blog is intended to encourage conversation on this difficult topic and challenge thinking. It is in no way intended to promote the use of physical restraint. I have never met anyone that enjoys physically restraining people, and if they do they are in the wrong job. However, there are some situations when there are no alternatives. I strongly support the premise of “restraint reduction”, but I intend to explain here why I believe that having the focus on reducing restraint will not be successful in achieving it and encourage sensible discussions on this further. I state further for clarity, this blog is not against the “restraint reduction” work that is making excellent progress, but aims to provide supportive considerations to help further progress work in this challenging area.
“Restraint reduction” implies “all restraint is bad”.
Physical restraint is usually used when people are extremely distressed. If physical restraint is not used then the person could be at risk of harming themselves or others. People come to work in social care because they are caring and want to make a difference. The negativity associated with physical interventions can lead to people feeling they are bad people for having to do these essential actions that they are doing in a caring way. It can make people think they have done things wrong, when they have done their best in that moment. This risks driving the caring people we want to attract into health and social care away, or drive these practices underground and make them more hidden. We need an open culture that acknowledges sometimes restraint is necessary.
Most of the time physical restraint is applied in a caring way and those applying the restraint are wanting to support the person during their highest point of distress. Physical restraint is the end point of a line of physical supports where the use of physical touch can be supportive. Applying the notion that “all restraint is bad” leads us away from sensible discussions that sometimes restraint is necessary and can be supportive.
What is “least restrictive” for you may be “most restrictive” for me.
Everyone is different, and there is no global hierarchy of what restraint is least restrictive. Some people may find physical contact extremely aversive, whilst others find physical contact comforting. I have supported people who will intentionally prompt being physically restrained in order to achieve the sensory feedback they achieve from this. I have also seen people who have needed 4:1 support due to “no touch” policies where physical support could have meant the person would be safe with 1 or 2 supporting. Is being supported by 4 people less restrictive than being supported by 1 person who can use physical restraint? Is physical restraint less restrictive than chemical restraint, mechanical restraint, or environmental restraint? Each person is different and will find different restraints more/less aversive than someone else. The only person who can really say what is “least restrictive” is the person receiving the restrictions.
For some people we support there can be risks to going out and trying new things. Sometimes, teaching teams in safe, respectful, physical interventions can give teams the courage and confidence to support people to go out and try new things. If the risk is that the person supported could do something that harms themselves or others and the team has no methods of supporting the person when these risks occur then the likelihood is that teams will take fewer positive risks. So the least restrictive option of not providing physical interventions can ultimately be more restrictive if it means people do not go out.
“Least restrictive” can sometimes be “least effective”.
There may be times when direct support is supporting someone in distress and a punch is heading their way and there is no alternative to physically holding someone. There is not time in situations like this to pull out a list of alternative things to try to do instead.
There is also the fable of “how to boil a frog”. The notion here is that if you put a frog in cold water and gently increase the temperature the frog will stay there, compared to if you expose a frog to boiling water it will jump out – please do not try this at home it is a fable and you should never try to boil a frog! However, the same notion here can be true for least restrictive approaches. Least restrictive methods may at times lead to events lasting for longer periods with the restrictions gradually increasing over time and may lead to situations where the end point is more restrictive than would have been if a more restrictive intervention was used to promptly and safely end the situation earlier. Least restrictive may at times therefore mean longer lasting, more distressing, and in the end more restrictive.
We should look to “replace” not “reduce”
We have learned from Positive Behaviour Support that if our only focus is on reducing behaviours then we miss the function of these behaviours. As a result, if you stop the behaviour you are focussing on then it is likely new behaviours will appear to meet these functions instead as the need has not been met. These new behaviours can be more challenging than the ones that were happening before.
If we treat physical interventions as a challenging behaviour, we know the same will be true. Focusing on reducing restraint will only lead to different, potentially more restrictive, interventions popping up. If we really want to reduce restraint we need to focus on what restraint is used for and we want to replace restraint with.
“Restraint reduction” is not a behaviour.
In Positive Behaviour Support we focus on what people do, not what people don’t do. People not doing things is not a behaviour. It is also very difficult to measure what doesn’t happen.
I often use the example of instead of saying “don’t walk on the grass” say “walk on the path”. If you say what you don’t want people to do then they do not know what is the positive expectation for them to do instead. If you say what you want people to do they are more likely to do it.
The position of “restraint reduction” therefore does not fit with what we know from the science of behaviour change. If we know the science works for the people we support, we know it works for the teams that support them too. We should not be taking the position of what we do not want support to do, we should be stating what behaviours we want to see people doing instead.
Approaches based on reduction, like restraint reduction, are by definition punishment.
The definition of punishment is an approach that reduces the likelihood that behaviour will happen in the future. Therefore, if our approach to restraint is to reduce it we are taking a punishment based approach towards restraint. We know that whilst punishment based approaches work, their effects are not as long standing as reinforcement based interventions and the quality of the outcomes are poorer. We also know that those who experience punishment based interventions can find them aversive.
Taking a punishment based approach to our teams supporting people sets the wrong conditions for creating cultures that avoid punishment based approaches with the people we support. We should use lessons learnt from Positive Behaviour Support and aim for positive reinforcement based approaches to develop alternative skills as our strategy to reduce restraint, instead of relying on punishment.
Concluding thoughts
I think there is merit in treating restraint like a challenging behaviour.
In Positive Behaviour Support we acknowledge that challenging behaviours challenge us, but they serve an important function for that person right now. We know simply aiming to reduce that behaviour is not the answer for long term change, and we miss our opportunity to understand what the behaviour is for and therefore the opportunity to teach that person new behaviours to replace the ones that challenge us. Teaching more effective behaviours makes challenging behaviours redundant as we empower people with better skills.
Similarly, without doubt, restraint is a challenging behaviour that we all want to reduce. Yet we know from the science of behaviour change that focussing on reduction alone is not the answer. The answer lies in understanding the function of this behaviour and using a multi-systemic approach to enabling teams to respond in alternative ways.
Whilst we should not ever stop our efforts to “reduce restraint” we do need to be able to have sensible conversations that sometimes restraint is necessary. Being able to discuss this will enable good practices to evolve. Driving these discussions underground, or not having these conversations at all, will not ensure there is safe, person centred practices when restraint is needed.
One final thought. This blog has largely focussed on how the term “restraint reduction” risks us putting our attention in the wrong place to achieve what we all collectively want. From April 2021 CQC will be expecting all providers to be using physical interventions that follow the Restraint Reduction Network standards. These standards are great progress in ensuring that when restraint is used it is done in a way that ensures peoples human rights are maintained and they are used safely. However, the standards are for the training packages. Is measuring training providers packages the right focus to ensure physical restraint is used safely or is our attention in the wrong place here too? My view would be that our focus should be on how those using the interventions are applying them. Purchasing a safe package does not ensure safe use of that package.

 A spoon is just a thing too. Generally spoons do good. They stir your tea, help you eat yoghurt, soup, cereal. You can balance them on your nose. See yourself upside down in them, play music with them. Generally a very useful thing. Sometimes spoons can be used for evil. If you don’t believe me just ask Richard Gale
A spoon is just a thing too. Generally spoons do good. They stir your tea, help you eat yoghurt, soup, cereal. You can balance them on your nose. See yourself upside down in them, play music with them. Generally a very useful thing. Sometimes spoons can be used for evil. If you don’t believe me just ask Richard Gale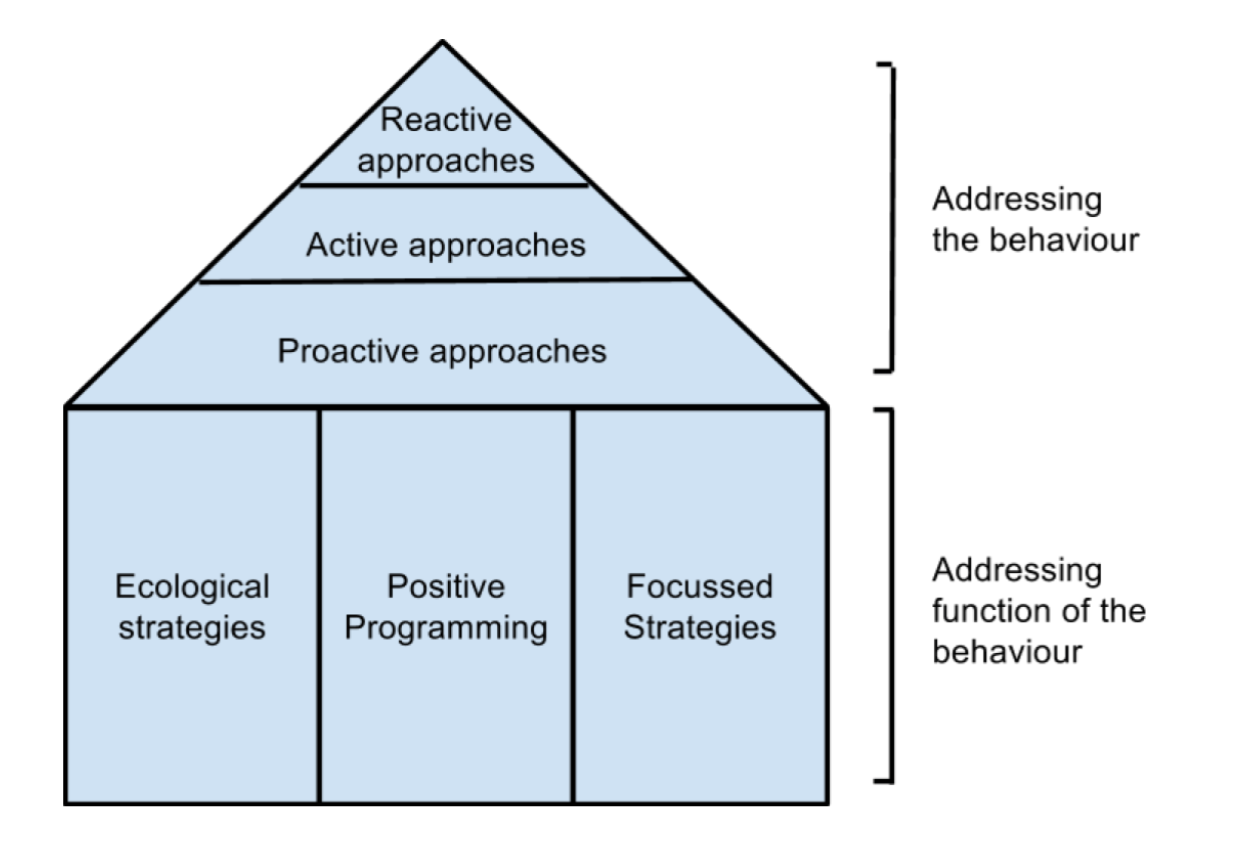

 What went well?
What went well?